MEASUREMENTS IN FITTING EYEGLASSES
For eyeglasses to be effective, patients must feel satisfied with the prescription and the overall fit of the lenses of the face. Eyeglasses that fit improperly may cause vision problems. To help determine the source of a patient's dissatisfaction or discomfort with eyeglasses, ophthalmic medical assistants may need to measure interpupillary distance, vertex distance, and the base curves of the lenses.
Interpupillary distance (abbreviated IPD or PD) is the distance from the center of the pupil of the other eye. IPD is important to the laboratory technician who makes eyeglass lenses because it indicates where to place the ground optical centers in the finished lenses so that they lie directly in front of the patient's pupils. The optical center of a lens denotes the point of optimal vision; it is the single point through which light may pass without making being bent or changed (Fig 1.1)

INTERPUPILLARY DISTANCE
Interpupillary distance, the distance between the pupils, is measured in millimeters. This measurement should be obtained both at near and at distance for each patient. Both a binocular measurement (a single recording of the total distance from pupil to pupil) and a monocular measurement (the individual distance from the center of the bridge of the nose to the center of each pupil) should be recorded.(Fig.1.2)

The distance IPD measurement is required to manufacture all eyeglasses, both single-vision and multifocal. The near IPD measurement is required when single-vision or multifocal eyeglasses are prescribed for reading or other close-up activities. The accurate measurement of both distance and near IPD ensures the appropriate placement of the optical centers of the eyeglass lenses. If the distance between optical centers (DBC) does not correspond to the patient's IPD, the patient can experience double vision. Therefore, the ophthalmic medical assistant should verify the correct IPD and DBC for all eyeglasses whether they are new prescriptions or eyeglasses brought in by patients with vision complaints.
Several methods exist for measuring distance or near IPD. In addition, either binocular or monocular measurements may be chosen. Monocular measurement of IPD is considered more accurate than binocular measurement because the monocular recording takes into consideration any facial asymmetry that might be present. (Fig 1.2)
A binocular distance IPD requires just one pupil-to-pupil measurement made with a millimeter ruler. For a monocular distance IPD measurement, the distances between each pupil and the bridge of the nose are measured separately and the results are added together to yield a single measurement. Simple and accurate monocular IPD measurements may be made with a specially caliberated ruler and a penlight. Specific instructions for both of these distance IPD measuring techniques are presented in the boxes "Measuring Binocular Distance IPD" and "Measuring Monocular Distance IPD" on separate section. IPD measurements can also be made with a corneal reflection pupilometer,discussed later.
Both binocular and monocular near IPD may be measured or calculated in Table presents the approximate near IPDs corresponding to a range of common monocular distance IPDs. Measuring the binocular or monocular near IPD requires both the millimeter ruler and the penlight. The box "Measuring Binocular Near IPD" contains step-by-step instructions for this technique. The monocular measuring technique for near IPD is not presented here because it requires more experience and skill than would be expected of an assistant.
ERRORS IN MEASURING IPD
The accurate measurement of both distance and near IPD ensures that the optical centers of the patient's eyeglass lenses are correctly placed in front of the patient's pupils. If the distance between optical centers (DBC) does not correspond to the measured IPD, an optical distortion known as prismatic effect may occur. Prismatic effect causes incoming light rays to deviate inappropriately when they strike the lens (Fig 1.3), leading to eye discomfort or disorted or double vision for the lens wearer. The direction of the prismatic effect can vary depending on whether a plus-power lens or minus-power lens is involved and on whether the DBC of the lens is wider or narrower than the IPD.
Several common errors can occur when using the millimeter ruler to measure distance and near IPD.

Special instruments, such as the Essilor Pupilometer, and other metering devices, are used to measure IPD(Fig 1.4). Opticians use them routinely because these meters correct for parallax error. In addition, the instruments provide a monocular reading that avoids errors due to facial asymmetry or strabismus. Because the operation of each instrument differs, ophthalmic medical assistants should read in detail the user's manual for the particular instrument available in their practice and request practical instruction in its use from the ophthalmologist or a senior staff assistant.

TABLE I - MEASURING BINOCULAR DISTANCE IPD
Gauging the precise center of a patient's pupils can be difficult, especially if the pupils are large. A reasonably accurate measurement can be obtained by measuring from the temporal limbus of one eye to the nasal limbus of the other eye.
1. Position yourself about 16 inches in front of the patient. Make sure your eyes are level with the patient's eyes.
2. Close your right eye and ask the patient to look at your left eye.
3. Rest the millimeter ruler lightly on the bridge of the patient's nose.
4. Line up the zero point on the temporal limbus of the patient's right eye (Figure A).
5. Holding the ruler in this position, close your left eye and open your right eye. Have the patient fixate on your right eye.
6. Observe the number on the millimeter ruler that is directly under the nasal limbus of the patient's left eye.(Figure B)
7. Close your right eye, open your left eye, and check the zero point of the ruler, making sure it is at the temporal limbus of the patient's right eye.
8. Check the measurement on the ruler for the patient's left eye and record it on the patient's chart or form as appropriate.


TABLE II - MONOCULAR DISTANCE IPD WITH CORRESPONDING AVERAGE NEAR IPD (mm)
DIST NEAR
24.75 23.00
25.25 23.50
25.75 24.00
26.25 24.50
26.75 25.00
27.25 25.50
27.75 26.00
28.50 26.50
29.00 27.00
29.50 27.50
30.00 28.00
30.50 28.50
31.00 29.00
31.50 29.50
32.00 30.00
32.75 30.50
33.25 31.50
33.75 31.50
34.25 32.00
34.75 32.50
35.25 33.00
36.00 33.50
36.50 34.00
37.00 34.50
TABLE III - MEASURING MONOCULAR DISTANCE IPD
1. Position yourself 14 to 16 inches infront of the patient. Make sure your eyes are level with the patient's eyes. Hold the millimeter ruler lightly over the bridge of the patient's nose.
2. Hold a penlight under your left eye, aiming the light at the patient's eye. Note the position of the spot of light reflection called the corneal reflex on the patient's right eye (see the figure), and record the number on the ruler just below the reflex. This represents the number of millimeters from the patient's right corneal reflex to the center of the bridge of the nose.
3. Hold the penlight under your right eye, aiming the light at the patient's eye. Observe the corneal reflex on the patient's left eye. Record the number of millimeters from the left corneal reflex to the center of the bridge of the nose.
4. Add the two numbers together and record the sum on the patient's chart or form as appropriate.

TABLE IV - MEASURING BINOCULAR NEAR IPD
1. Place your dominant eye in front of the patient's nose at the patient's near working distance, which is usually 14 to 16 inches.
2. Close your other eye and have the patient fixate on your open eye (your dominant eye).
3. Rest the millimeter ruler lightly on the bridge of the patient's nose and line up the zero point at the center of the patient's right pupil.
4. Record the reading from the ruler marking at the center of the patient's left pupil.
5. Hold the penlight directly under your right eye and shine the ligth toward the patient's nose. A crisp corneal reflection on both eyes will be seen. This may help you in making these measurements because the light reflex is the center of the cornea (and almost the center of the pupil), and you can determine a reading on the millimeter scale by reading from the ruler at the corneal reflex.
Vertex Distance and Base curve measurement, we will explore in further post.

For eyeglasses to be effective, patients must feel satisfied with the prescription and the overall fit of the lenses of the face. Eyeglasses that fit improperly may cause vision problems. To help determine the source of a patient's dissatisfaction or discomfort with eyeglasses, ophthalmic medical assistants may need to measure interpupillary distance, vertex distance, and the base curves of the lenses.
Interpupillary distance (abbreviated IPD or PD) is the distance from the center of the pupil of the other eye. IPD is important to the laboratory technician who makes eyeglass lenses because it indicates where to place the ground optical centers in the finished lenses so that they lie directly in front of the patient's pupils. The optical center of a lens denotes the point of optimal vision; it is the single point through which light may pass without making being bent or changed (Fig 1.1)

Fig 1.1 Relationship of the optical center of the eyeglass lens to the pupil
The vertex distance is the distance from the back surface of an eyeglass lens to the surface of the patient's cornea. This measurement can be an important factor in making eyeglasses with powers greater than plus or minus 5, because at higher powers the distance from the eye can change the effective power of a lens. The base curve is the curve of the lens surface, usually the outer or front side of the lens, from which the other curves necessary for sight correction are calculated.INTERPUPILLARY DISTANCE
Interpupillary distance, the distance between the pupils, is measured in millimeters. This measurement should be obtained both at near and at distance for each patient. Both a binocular measurement (a single recording of the total distance from pupil to pupil) and a monocular measurement (the individual distance from the center of the bridge of the nose to the center of each pupil) should be recorded.(Fig.1.2)

Fig 1.2 Relationship of binocular and monocular measurements for interpupillary distance
In orthophoric (normal) patients, the eyes look straight ahead when they focus on an object directly in front of them. Eyes that are straight in the primary gaze (straight ahead) will have virtually parallel axes when they fixate on a distant object. However, when the same pair of eyes focuses on a near object, the eyes converge (turn in slightly) to allow both foveas to fixate at the object. Because of this convergence, the near IPD measurement will be less than the distance IPD.The distance IPD measurement is required to manufacture all eyeglasses, both single-vision and multifocal. The near IPD measurement is required when single-vision or multifocal eyeglasses are prescribed for reading or other close-up activities. The accurate measurement of both distance and near IPD ensures the appropriate placement of the optical centers of the eyeglass lenses. If the distance between optical centers (DBC) does not correspond to the patient's IPD, the patient can experience double vision. Therefore, the ophthalmic medical assistant should verify the correct IPD and DBC for all eyeglasses whether they are new prescriptions or eyeglasses brought in by patients with vision complaints.
Several methods exist for measuring distance or near IPD. In addition, either binocular or monocular measurements may be chosen. Monocular measurement of IPD is considered more accurate than binocular measurement because the monocular recording takes into consideration any facial asymmetry that might be present. (Fig 1.2)
A binocular distance IPD requires just one pupil-to-pupil measurement made with a millimeter ruler. For a monocular distance IPD measurement, the distances between each pupil and the bridge of the nose are measured separately and the results are added together to yield a single measurement. Simple and accurate monocular IPD measurements may be made with a specially caliberated ruler and a penlight. Specific instructions for both of these distance IPD measuring techniques are presented in the boxes "Measuring Binocular Distance IPD" and "Measuring Monocular Distance IPD" on separate section. IPD measurements can also be made with a corneal reflection pupilometer,discussed later.
Both binocular and monocular near IPD may be measured or calculated in Table presents the approximate near IPDs corresponding to a range of common monocular distance IPDs. Measuring the binocular or monocular near IPD requires both the millimeter ruler and the penlight. The box "Measuring Binocular Near IPD" contains step-by-step instructions for this technique. The monocular measuring technique for near IPD is not presented here because it requires more experience and skill than would be expected of an assistant.
ERRORS IN MEASURING IPD
The accurate measurement of both distance and near IPD ensures that the optical centers of the patient's eyeglass lenses are correctly placed in front of the patient's pupils. If the distance between optical centers (DBC) does not correspond to the measured IPD, an optical distortion known as prismatic effect may occur. Prismatic effect causes incoming light rays to deviate inappropriately when they strike the lens (Fig 1.3), leading to eye discomfort or disorted or double vision for the lens wearer. The direction of the prismatic effect can vary depending on whether a plus-power lens or minus-power lens is involved and on whether the DBC of the lens is wider or narrower than the IPD.
Several common errors can occur when using the millimeter ruler to measure distance and near IPD.

Fig 1.3 Prismatic effect in a minus-power lens for which the distance between optical centers (DBC) is narrower than the interpupillary distance (IPD)
Some errors in measurement relate to a patient's strabismus or asymmeteric face. The most common cause of error in assessing IPD is parallax, an optical disortion that occurs when the measurer's and the patient's lines of sight are not parallel. Parallax can result in the measured IPD being significantly different from the patient's actual IPD. It can result from the measurer standing closer to the patient than 14 inches; from head movement by the measurer or patient; from improper eye fixation by the patient during the measurement; or from the examiner's line of sight being higher or lower than the patient's.Special instruments, such as the Essilor Pupilometer, and other metering devices, are used to measure IPD(Fig 1.4). Opticians use them routinely because these meters correct for parallax error. In addition, the instruments provide a monocular reading that avoids errors due to facial asymmetry or strabismus. Because the operation of each instrument differs, ophthalmic medical assistants should read in detail the user's manual for the particular instrument available in their practice and request practical instruction in its use from the ophthalmologist or a senior staff assistant.

Fig 1.4 Essilor Pupilometer used to measure interpupillary distance.
TABLE I - MEASURING BINOCULAR DISTANCE IPD
Gauging the precise center of a patient's pupils can be difficult, especially if the pupils are large. A reasonably accurate measurement can be obtained by measuring from the temporal limbus of one eye to the nasal limbus of the other eye.
1. Position yourself about 16 inches in front of the patient. Make sure your eyes are level with the patient's eyes.
2. Close your right eye and ask the patient to look at your left eye.
3. Rest the millimeter ruler lightly on the bridge of the patient's nose.
4. Line up the zero point on the temporal limbus of the patient's right eye (Figure A).
5. Holding the ruler in this position, close your left eye and open your right eye. Have the patient fixate on your right eye.
6. Observe the number on the millimeter ruler that is directly under the nasal limbus of the patient's left eye.(Figure B)
7. Close your right eye, open your left eye, and check the zero point of the ruler, making sure it is at the temporal limbus of the patient's right eye.
8. Check the measurement on the ruler for the patient's left eye and record it on the patient's chart or form as appropriate.

Figure A

Figure B
DIST NEAR
24.75 23.00
25.25 23.50
25.75 24.00
26.25 24.50
26.75 25.00
27.25 25.50
27.75 26.00
28.50 26.50
29.00 27.00
29.50 27.50
30.00 28.00
30.50 28.50
31.00 29.00
31.50 29.50
32.00 30.00
32.75 30.50
33.25 31.50
33.75 31.50
34.25 32.00
34.75 32.50
35.25 33.00
36.00 33.50
36.50 34.00
37.00 34.50
TABLE III - MEASURING MONOCULAR DISTANCE IPD
1. Position yourself 14 to 16 inches infront of the patient. Make sure your eyes are level with the patient's eyes. Hold the millimeter ruler lightly over the bridge of the patient's nose.
2. Hold a penlight under your left eye, aiming the light at the patient's eye. Note the position of the spot of light reflection called the corneal reflex on the patient's right eye (see the figure), and record the number on the ruler just below the reflex. This represents the number of millimeters from the patient's right corneal reflex to the center of the bridge of the nose.
3. Hold the penlight under your right eye, aiming the light at the patient's eye. Observe the corneal reflex on the patient's left eye. Record the number of millimeters from the left corneal reflex to the center of the bridge of the nose.
4. Add the two numbers together and record the sum on the patient's chart or form as appropriate.
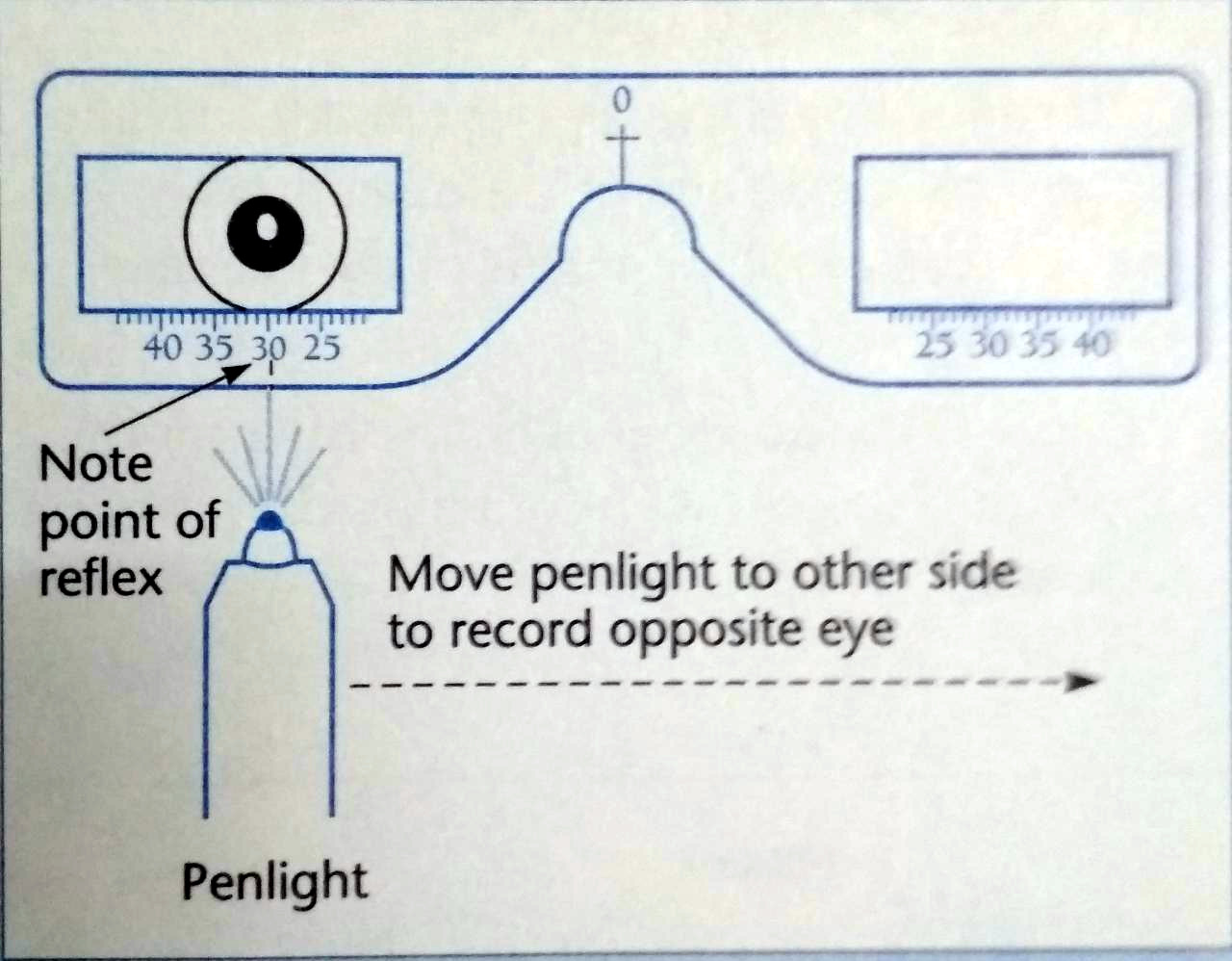
Figure. Measuring Monocular Distance IPD
TABLE IV - MEASURING BINOCULAR NEAR IPD
1. Place your dominant eye in front of the patient's nose at the patient's near working distance, which is usually 14 to 16 inches.
2. Close your other eye and have the patient fixate on your open eye (your dominant eye).
3. Rest the millimeter ruler lightly on the bridge of the patient's nose and line up the zero point at the center of the patient's right pupil.
4. Record the reading from the ruler marking at the center of the patient's left pupil.
5. Hold the penlight directly under your right eye and shine the ligth toward the patient's nose. A crisp corneal reflection on both eyes will be seen. This may help you in making these measurements because the light reflex is the center of the cornea (and almost the center of the pupil), and you can determine a reading on the millimeter scale by reading from the ruler at the corneal reflex.
Vertex Distance and Base curve measurement, we will explore in further post.
Comments
Post a Comment